
Magnetic-assisted surgery: the road from laparoscopy to robotics
 0
0 , ...
, ... Abstract
The incorporation of magnetic fields into surgery to reduce the invasiveness of minimally invasive surgery led to the creation of magnetic-assisted surgery. External magnets coupled with their internal counterparts assist during surgical procedures, avoiding the need for additional trocars. Multiple advances have been made in this field in the past 15 years, with new promising technologies being developed. This review centers on the history of
Keywords
INTRODUCTION
The beginnings of minimally invasive surgery (MIS) can be traced back to the twentieth century[1]. The first MIS procedures were an appendectomy by Semm in 1982 and a cholecystectomy by Muhe in 1985[2]. Although there was not much attention or acceptance during the first years, they turned out to be the standard of care in the following decades[3,4]. Over time, MIS has demonstrated good surgical outcomes and a quicker recovery[5]. MIS is an evolving field with emerging techniques and technologies in an attempt to decrease the traumatic insult to the body that surgery represents. Based on these principles, the field of magnetic-assisted laparoscopic surgery was first established[6,7].
Magnetism is a physical property of certain metals which produces either a pulling or a pushing force between two objects. The existence of natural magnets (Fe3O4) has been known to humankind for thousands of years[8]. However, the most primitive records show that the application of these electrical properties into medicine was likely introduced by the ancient Hindus, who used them to remove foreign bodies beneath the skin[9]. Since then, the inclusion of magnetic fields in medicine has expanded with multiple diagnostic and therapeutic uses[10]. In fact, magnetic surgery includes but is not limited to magnetic compression anastomosis (Magnamosis), magnetic anchoring technique, magnetic navigation technique, magnetic sphincter augmentation, self-assembling magnets for endoscopic intestinal bypass, magnetic compression ostomy, and correction of congenital deformities[11]. For the purpose of the current manuscript, magnetic-assisted surgery will be used in relation to magnetic anchoring technique.
Looking at the long history of magnetism in medicine and surgery, its incorporation into MIS is relatively new. While MIS has already proven to decrease pain, given its relatively small incisions compared to open surgery, it still involves an insult to the body. Motivated to further decrease the transgression to the body, researchers have developed the concept of magnetic-assisted surgery in the past years. The advantage of this technology is to provide the same traction and counter-retraction necessary during surgery without making additional incisions. This review will describe the timed development of the technology through the different studies summarized in Table 1.
Current publications of magnetic surgery
| Author | Year | Country | Surgery | Design | n | Conclusion |
| Park et al.[6] | 2007 | USA | Laparoscopic nephrectomy | Porcine model | 2 | Trocar-less laparoscopy using magnetically anchored instruments is feasible |
| Dominguez[7] | 2007 | Argentina | Laparoscopic cholecystectomy | Case report | 1 | Magnetic instruments can provide traction and counter traction |
| Scott et al.[12] | 2007 | USA | Transvaginal cholecystectomy | Porcine model | 4 | Magnetic surgery is under development but feasible. |
| Kume et al.[13] | 2008 | Japan | Laparoscopic cholecystectomy | Porcine model | 1 | Magnet-retracting forceps provide port-less access to the abdominal cavity |
| Kume et al.[14] | 2008 | Japan | Laparoscopic anterior resection | Porcine model | 1 | Endoluminal magnetic anchors provide effective retraction |
| Dominguez et al.[15] | 2009 | Argentina | Laparoscopic cholecystectomy | Case series | 40 | Triangulation with forceps controlled by magnetic fields appears to be feasible and safe |
| Morales-Conde et al.[16] | 2011 | Spain | Laparoscopic sleeve gastrectomy | Case report | 1 | Single-port approach with the aid of magnetic forceps is feasible and safe in expert hands |
| Martinez-Ferro et al.[17] | 2012 | Argentina | Laparoscopic Nissen | Case report | 1 | Nissen fundoplication with magnetic guidance is a feasible procedure |
| Rivas et al.[18] | 2016 | Chile | Laparoscopic cholecystectomy | Prospective single arm | 50 | Safe and feasible |
| Haskins et al.[19] | 2017 | USA | Laparoscopic cholecystectomy | Case series | 10 | Safe, feasible and reduces the number of trocars |
| Guerron | 2017 | USA | Robotic-assisted cholecystectomy | Case report | 1 | Combination of robot and magnetic surgery is feasible |
| Davalos et al.[21] | 2019 | USA | Laparoscopic right colectomy Laparoscopic sigmoidecomy Laparoscopic rectopexy | Case series | 10 | Safe, dynamic and incision-less |
| Davis et al.[22] | 2019 | USA | Laparoscopic sleeve gastrectomy Laparoscopic RYGB Laparoscopic BPD-DS Laparoscopic revision Laparoscopic band removal | Retrospective | 73 | Device successfully permitted optimal liver retraction while decreasing the number of abdominal incisions |
| Steinberg | 2018 | USA | Robot-assisted radical prostatectomy | Case series | 3 | Safe and effective retraction Reduce the number of ports |
| Steinberg | 2019 | USA | Reduced port robotic-assisted radical prostatectomy | Case series | 16 | Magnetic system avoids the need for a 4th robotic arm Safe and effective |
| Steinberg | 2019 | USA | Single port robotic-assisted radical prostatectomy | Retrospective | 15 | Magnetic retractor facilitates tissue exposure and improves procedure ergonomics mimicking multiport technique |
| Luengas et al.[23] | 2020 | Chile | Laparoscopic sleeve gastrectomy Laparoscopic RYGB Laparoscopic BPD-DS Laparoscopic Revision | Prospective single arm | 50 | Adequate retraction, well tolerated and avoids epigastric incision |
| Barajas-Gamboa | 2020 | Chile | Laparoscopic cholecystectomy | Case series | 10 | Novel combination of magnetic and robotic technologies is safe and feasible |
| Ganesan | 2020 | USA | Robotic-assisted sacrocolpopexy | Case series | 3 | Magnet eliminates the need for an additional trocar |
| Fulla et al.[30] | 2020 | USA | Robotic partial nephrectomy Robotic radical nephrectomy Robotic pyeloplasty Laparoscopic donor nephrectomy Laparoscopic radical nephrectomy | Prospective single arm | 10 | Safe and feasible. Useful to expose the renal hilum |
| Huang et al.[28] | 2020 | USA | Robotic-assisted prostatectomy | Retrospective | 39 | Safe and reproducible tissue retraction while not requiring additional incisions |
| Roberts et al.[24] | 2020 | USA | Laparoscopic sleeve gastrectomy | Retrospective | 50 | Same-day discharge magnetic sleeve gastrectomy is safe and feasible |
| Welsh et al.[34] | 2021 | USA | Laparoscopic sleeve gastrectomy Laparoscopic RYGB Laparoscopic BPD-DS | Retrospective case-control | 100 | Lower pain score at 12 h Lower length of stay Higher OR supply cost |
| Chen et al.[31] | 2021 | China | Thoracoscopic Esophagectomy | Porcine model | 10 | Magnetic anchoring and traction system is safe and feasible |
| Fu et al.[32] | 2022 | China | Thoracoscopic Esophagectomy | Prospective single arm | 10 | Magnetic anchoring and traction system can improve the exposure of RLN |
IN-VIVO ANIMAL MODELS
In 2007, Park and Cadeddu, described the “magnetic anchoring and guidance system” (MAGS), which was tested in a porcine laparoscopic surgery model[6]. Their prototype consisted of a stack of
The same investigators later employed MAGS to perform transvaginal cholecystectomies in porcine models[12]. Due to instrumentation shortcomings, two of their four procedures had to be ended prematurely. The authors mentioned that there was suboptimal retraction and inadvertent magnetic coupling between the instruments, which were solved by the learning curve in later cases. Nevertheless, they concluded that MAGS platform facilitated tissue triangulation, making magnetic-assisted surgery feasible but under development.
An independent group in Japan used an outer 3.9 cm coupled with an inner 1.0 cm Nd2Fe14B magnet to complete a porcine laparoscopic cholecystectomy and a laparoscopic anterior resection[13,14]. In their experiment, the extracorporeal magnet was moved on the abdominal wall, changing the position of the intra-peritoneal magnet and providing variable traction of the gallbladder. Importantly, the study describes that the magnet did not interfere with the vital signs monitoring of the pig nor with the electro-surgical instruments. The shortcomings of this technology raised by the authors were the susceptibility of neodymium to corrosion, which could pose a risk to the human body, and the potential interactions between magnets and other surgical instruments.
FIRST CLINICAL APPLICATION
The first reported clinical application of magnetic-assisted surgery in the literature was by Dominguez in 2007[7]. In this original report, a series of Nd2Fe14B magnets attached to an alligator grasper (TD-magnet) were used to retract the gallbladder fundus and infundibulum during a laparoscopic cholecystectomy. The inner magnets are controlled with external magnets to achieve triangulation. The surgery was done in
Further on, Morales-Conde et al. reported the first case of a single-port laparoscopic sleeve gastrectomy using the TD-magnet for retraction[16]. The case involved a 51-year-old female with a BMI of 45 kg/m2. Using a 2.5 cm transverse incision with the assistance of the magnets for proper traction and triangulation, the authors were able to complete the surgery in 120 min without the need for additional trocars. No perioperative or postoperative complications were reported. The authors concluded that surgery using magnetic forceps is feasible and safe in the hands of experienced laparoscopic surgeons. In a similar fashion and without complications, a laparoscopic Nissen fundoplication was performed using a single incision with the adjunct of magnetic forceps[17].
FIRST PROSPECTIVE CLINICAL TRIAL
These prototypes established the initial basis of magnetic-assisted surgery, but more adjustments were still to come. The first clinical trial of the Magnetic Surgical System (MSS) [Figure 1] by Levita Magnetics Corp. (Menlo Park, CA) took place from January 2014 to March 2015[18]. MSS consists of an external reusable magnet and a single-use grasper with a detachable magnetic tip that provides dynamic retraction. The instrument is compatible with a 10 mm trocar, and once it is attached to the target organ, the tip is released and coupled with the external magnet providing traction for the desired intervention. In a study by
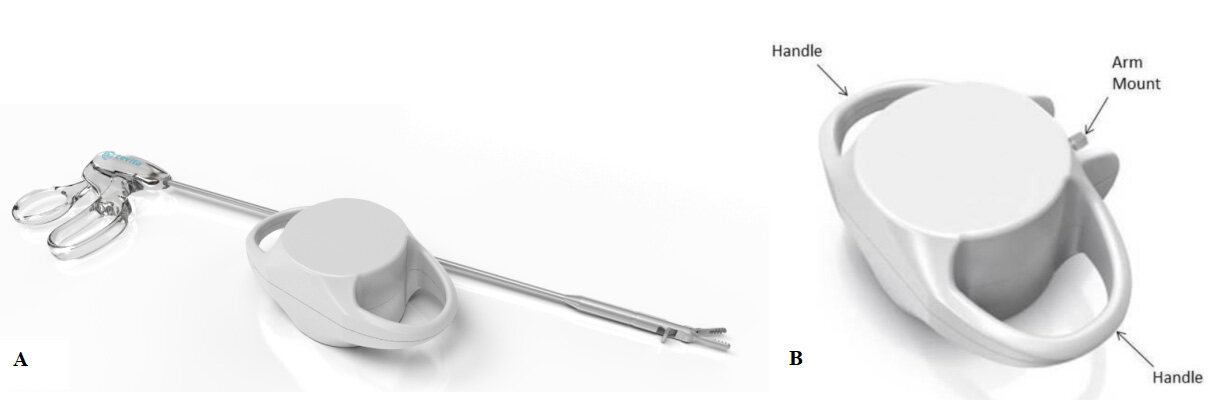
Figure 1. Magnetic surgical system (Levita Magnetics, Menlo Park, CA). (A) Magnetic grasper. (B) Magnetic controller. Reproduced with permission of Levita Magnetics.
A total of 50 patients with a mean BMI of 27 kg/m2 underwent a 3-port laparoscopic cholecystectomy with the assistance of the MSS at three different hospitals. The average procedure time was 63 min, with 90% of the surgeons reporting “excellent” exposure. There were no device malfunctions, major complications, or serious adverse events related to the device. Although no external abdominal wall abnormalities were noted, in 38% of the patients, internal petechiae were noted and presumed to be related to the magnetic device without clinical significance. The authors concluded that MSS is safe and feasible as the study met the outlined endpoint criteria[18].
FIRST APPLICATION IN THE UNITED STATES
In 2017 the Food and Drug Administration (FDA) cleared the use of the Levita MSS for laparoscopic cholecystectomy in patients with a BMI range of 20 to 34 kg/m2 (DEN150007/K171429). After that, the first case series in the US was reported by Haskins and Kroh[19]. A total of ten patients with a mean BMI of
Guerron et al. employed for the first time the MSS in conjunction with the da Vinci Single-Port platform (Intuitive Surgical, Sunnyvale, CA)[20]. In their case report, a 48-year-old patient with a BMI of 33 kg/m2 underwent a robotic-assisted cholecystectomy in 58 min. No operative complications were reported and the patient was discharged home the same day. The authors concluded that the combination of technologies was feasible, and the addition of the magnetic retractor helped overcome the challenges of single-port robotic surgery by incorporating shaftless interaction and collision.
These first reports using MSS in the US noted some limitations of this new technology that prompted further studies in the area. One of them was the narrow criteria for using the magnetic retractor[19]. The second disadvantage in cholecystectomy was associated with a higher BMI and related increased abdominal wall thickness, as well as the known decreased coupling strength with increasing distance from prior studies[6,20].
SHIFTING BEYOND GALLBLADDER
Davalos et al. reported a case series of laparoscopic colorectal procedures where the MSS was used[21]. Four single-port right colectomies, one sigmoidectomy, and five rectopexies were done consecutively using the magnetic grasper. The device successfully assisted with the retraction of the colon, uterus and mesentery. For the first time, two patients in the series had a BMI > 34 kg/m2; in one of them, the surgery was converted to open due to dense adhesions. Although the operative time was marginally longer, the authors attributed this to the learning curve inherent to a new technology.
A retrospective study by Davis et al. evaluated the use of MSS in bariatric surgery[22]. A total of 63 primary surgeries and 10 revisions were included, with a mean BMI of 43.6 kg/m2. The magnetic device was used to retract the liver. The surgeons were able to set up the device with adequate liver retraction in less than
Urology is another field that has incorporated MSS into its practice. Four studies reported the adjunct use of magnetic-assisted surgery during robotic-assisted radical prostatectomies[25-28]. A total of 31 patients from two institutions underwent the procedures without associated adverse outcomes or compromise of the fundamental steps of the procedure. MSS allowed the sparing of the 4th robotic arm in all of the surgeries. The magnetic retractor was used to retract the colon, bladder, and seminal vesicles, with no crush injuries noted on the tissues[27]. Nevertheless, the surgeons reported weaker magnetic coupling related to an increased body wall thickness in two patients with BMI > 35 kg/m2[25].
Other applications of magnetic retraction using MSS include robotic-assisted laparoscopic sacrocolpopexy, robotic-assisted partial nephrectomies, robotic-assisted pyeloplasty, laparoscopic radical nephrectomy and laparoscopic donor nephrectomy[29,30]. In these studies, no adverse events have been reported and the authors recognized adequate exposure during dissection.
As the field of magnetic-assisted surgery has evolved, newer adaptations have emerged. These evolutions have expanded beyond the field of abdominal surgery. In fact, its use in thoracic surgery has also been described. Chen et al. described the use of the magnetic anchoring and traction system (MATS) to facilitate esophageal dissection in a porcine model[31]. This system is composed of an external unit of
A follow-up study by the same group proved the safety and feasibility of MATS in vivo[32]. In a prospective way, ten patients undergoing thoracoscopic esophagectomy were enrolled. All of the patients underwent surgery with MATS, providing retraction of the proximal esophagus. The authors report that the traction provided by MATS allowed them to identify the recurrent laryngeal nerve adequately. This study provided further evidence that the use of magnetic-assisted surgery reduces the trauma to the chest wall. However, certain limitations including the possibility of magnetization of the internal cylinder and the loss of coupling were noted, which warrant further improvements of this novel system.
FOLLOW-UP CLINICAL TRIALS
The increased use and applicability of the MSS provoked further controlled studies to evaluate the safety and effectiveness of the device in different populations. A prospective, single-arm study included 50 patients undergoing bariatric surgery at two centers[23]. The mean BMI of the study population was 40.7 kg/m2, with the majority of them undergoing sleeve gastrectomy. In all of the cases, MSS provided adequate liver mobilization with an average time of 1 min to be deployed. A total of 22 mild adverse events were reported related to the device, including peritoneal petechiae and a minor liver capsule abrasion. Two major events occurred during the study unrelated to the subject device. In April 2020, the FDA approved the use of MSS in patients with BMI 20-60 kg/m2[33].
While the safety and feasibility of magnetic-assisted surgery been studied in different procedures, the question of its sustained benefit is still a matter of debate. A retrospective case-matched comparison between MSS and an external retractor was made by Welsh et al.[34]. In this study, 100 patients operated with MSS were compared to 196 matched historical controls using the Nathanson retractor. The former had lower pain scores at 12 h (2.9 vs. 3.8; P = 0.004) and lower length of stay (LOS) (1.5 vs. 1.8 days; P = 0.0051). The results of this study are the first data confirming the clinical benefit of the use of magnetic-assisted surgery in terms of pain reduction and its link to decreased LOS.
FUTURE DIRECTIONS AND LIMITATIONS
One of the main limitations of magnetic-assisted surgery is the fact that the coupling strength of the magnets decreases as a decaying exponential with respect to the distance between the source magnet and its target[6]. Although this inconvenience was first noted during the animal trials, other groups have accounted for it when used in patients with higher BMI as they tend to have thicker abdominal walls[25]. Interestingly, in the studies of MATS, the attraction force measured (in Newtons) was compared to the distance between the magnets in millimeters[31,32]. In the study graphs, it can be seen that with a distance of 80 mm, the force of the magnets is minimal, which can account for the loss of coupling seen in patients with thicker abdominal walls. However, in the study by Luengas et al., the device was able to be used in patients with a BMI up to 58 kg/m2[23]. These differences might be explained by different strengths of the magnets employed in each study. Set this limitation and the fact that using the same energy for all patients could then, on the other hand, predispose to excessive trauma to the tissues; future technologies may allow applying a tailored force to the distance between the magnets.
The combination of magnetic technologies in robotic cases has decreased the need for extra robotic arms in standard robotic procedures and assisted in the performance of single-port robotic surgery[25,29,30]. Nevertheless, the MSS still requires manipulation by an assistant at the bedside. This limitation further pushed the development of an integrated system. Barajas-Gamboa et al. published the first 10 case series using a Magnetic-Robotic Controller (Levita Magnetics, Menlo Park, CA)[35]. This system incorporates one robotic arm to control the external magnet to manipulate tissue in real time without the need for an additional assistant. The device is in the sterile field and controlled by the operating surgeon. In this study, all patients successfully underwent a reduced ports laparoscopic cholecystectomy (3 ports avoiding the epigastric incision) in addition to the robotically controlled magnetic grasper. No adverse events were reported and no unintentionally decoupling of the magnets occurred. The authors concluded that the integration of magnetic and robotic surgery was feasible as a proof of concept.
As a next step, a fully robotic magnetic platform was developed by Levita Magnetics [Figure 2]. The concept behind this is to empower the surgeon to perform the surgeries without any other assistant than the robot while providing a less invasive procedure with magnetic-assisted surgery. This disruptive approach to robotics is under evaluation in clinical trials (ClinicalTrials.gov Identifier: NCT05353777) and is expected to be ready for clinical use soon. The motivation is to bring benefits to the patients with a reduced incision technique, increase control and visualization to the surgeon and increase the efficiency of the providers.
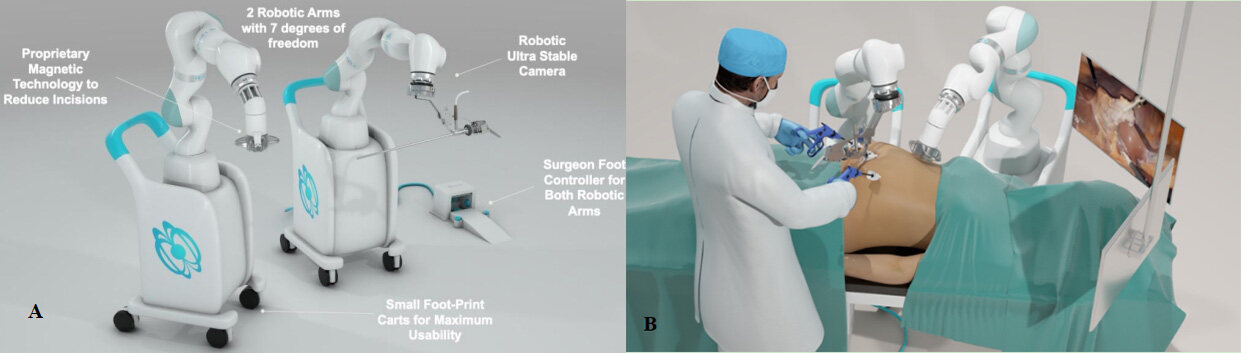
Figure 2. Magnetic-Robotic Controller (Levita Magnetics, Menlo Park, CA). (A) Console with robotic magnetic arms. (B) Schematization of the use of the platform. Reproduced with permission of Levita Magnetics.
CONCLUSIONS
Magnetic-assisted surgery is an extremely promising technology that will further decrease the invasiveness of minimally invasive surgery. Although most studies have shown its safety and feasibility, future studies should be aimed to confirm its wider clinical benefits compared to standard treatments in different procedures. Therefore, the combination of robotics and magnetic-assisted surgery is a very logical next step to bring benefits to patients, surgeons and providers.
DECLARATIONS
Author’s contributionsPerformed the literature review and draft the manuscript: Romero-Velez G, Portenier D
Reviewed the manuscript: Rodriguez-Navarro A, Roberts J, Oviedo RJ
Reviewed, edited the manuscript and guarantor the article: Kroh M
Availability of data materialsNot applicable.
Financial support and sponsorshipNone.
Conflicts of interestRodriguez-Navarro A: Founder of Levita Magnetics. Other authors declared that there are no conflicts of interest.
Ethical approval and consent to participateNot applicable.
Consent for publicationNot applicable.
Copyright© The Author(s) 2022.
REFERENCES
1. Vecchio R, MacFayden BV, Palazzo F. History of laparoscopic surgery. Panminerva Med 2000;42:87-90.
2. Litynski GS. Erich Mühe and the rejection of laparoscopic cholecystectomy (1985): a surgeon ahead of his time. JSLS 1998;2:341-6.
3. Minné L, Varner D, Burnell A, Ratzer E, Clark J, Haun W. Laparoscopic vs open appendectomy. Prospective randomized study of outcomes. Arch Surg 1997;132:708-11; discussion 712.
4. Southgate E, Vousden N, Karthikesalingam A, Markar SR, Black S, Zaidi A. Laparoscopic vs open appendectomy in older patients. Arch Surg 2012;147:557-62.
5. Epstein AJ, Groeneveld PW, Harhay MO, Yang F, Polsky D. Impact of minimally invasive surgery on medical spending and employee absenteeism. JAMA Surg 2013;148:641-7.
6. Park S, Bergs RA, Eberhart R, Baker L, Fernandez R, Cadeddu JA. Trocar-less instrumentation for laparoscopy: magnetic positioning of intra-abdominal camera and retractor. Ann Surg 2007;245:379-84.
7. Domínguez GM. . Colecistectomía con un trócar asistida por imanes de neodimio. Reporte de un caso. Available from: https://media2.supermagnete.hu/projects/pu450.pdf [Last accessed on 17 Oct 2022]
9. McCasiil MF. An improved hand electromagnet for eye surgery. Trans Am Ophthalmol Soc 1958;56:571-605.
10. Yuksel C, Ankarali S, Yuksel NA. The use of neodymium magnets in healthcare and their effects on health. North Clin Istanb 2018;5:268-73.
11. Lv Y, Shi Y. Scientific Committee of the First International Conference of Magnetic Surgery*. Xi’an consensus on magnetic surgery. Hepatobiliary Surg Nutr 2019;8:177-8.
12. Scott DJ, Tang SJ, Fernandez R, et al. Completely transvaginal NOTES cholecystectomy using magnetically anchored instruments. Surg Endosc 2007;21:2308-16.
13. Kume M, Miyazawa H, Abe F, et al. A newly designed magnet-retracting forceps for laparoscopic cholecystectomy in a swine model. Minim Invasive Ther Allied Technol 2008;17:251-4.
14. Kume M, Miyazawa H, Iwasaki W, Abe F, Uchinami H, Yamamoto Y. The use of magnetic anchors in the bowel lumen for laparoscopic anterior resection of rectosigmoid colon in pigs: with video. World J Surg 2008;32:2425-8.
15. Dominguez G, Durand L, De Rosa J, Danguise E, Arozamena C, Ferraina PA. Retraction and triangulation with neodymium magnetic forceps for single-port laparoscopic cholecystectomy. Surg Endosc 2009;23:1660-6.
16. Morales-Conde S, Dominguez G, Gomez JC, et al. Magnetic-assisted single-port sleeve gastrectomy. Surg Innov 2013;20:NP9-11.
17. Martinez-ferro M, Dominguez G, Millán C. Single-incision laparoscopic nissen fundoplication with adjunctive magnetic guidance. J Laparoendosc Adv Surg Tech Part B Videoscop 2012;22:6.
18. Rivas H, Robles I, Riquelme F, et al. Magnetic surgery: results from first prospective clinical trial in 50 patients. Ann Surg 2018;267:88-93.
19. Haskins IN, Strong AT, Allemang MT, Bencsath KP, Rodriguez JH, Kroh MD. Magnetic surgery: first U.S. experience with a novel device. Surg Endosc 2018;32:895-9.
20. Guerron AD, Ortega CB, Park C, Portenier D. . Magnetic robot-assisted single-incision cholecystectomy. Available from: https://crsls.sls.org/wp-content/uploads/2018/09/jls101183674001.pdf [Last accessed on 17 Oct 2022]
21. Davalos G, Lan BY, Diaz R, et al. Single-center experience with magnetic retraction in colorectal surgery. J Laparoendosc Adv Surg Tech A 2019;29:1033-7.
22. Davis M, Davalos G, Ortega C, et al. Magnetic liver retraction: an incision-less approach for less invasive bariatric surgery. Obes Surg 2019;29:1068-73.
23. Luengas R, Galindo J, Castro M, et al. First prospective clinical trial of reduced incision bariatric procedures using magnetic liver retraction. Surg Obes Relat Dis 2021;17:147-52.
24. Roberts J, Snow R, Novack R, Hall A, Smith A. Same day discharge magnetic sleeve gastrectomy: first 50 cases. Obesity 2020;28:40-187.
25. Steinberg RL, Johnson BA, Cadeddu JA. Magnetic-assisted robotic surgery: initial case series of reduced-port robotic prostatectomy. J Robot Surg 2019;13:599-603.
26. Steinberg RL, Johnson BA, Cadeddu JA. Magnetic-assisted robotic surgery to facilitate reduced-port radical prostatectomy. Urology 2019;126:237.
27. Steinberg RL, Johnson BA, Meskawi M, Gettman MT, Cadeddu JA. Magnet-assisted robotic prostatectomy using the da VINCI SP robot: an initial case series. J Endourol 2019;33:829-34.
28. Huang SF, Welsh LK, Davalos G, Houser RE, Rothman JR, Guerron DA. Robotic assisted prostatectomy with magnetic retraction. Urol Pract 2020;7:391-6.
29. Ganesan V, Goueli R, Rodriguez D, Hess D, Carmel M. Single-port robotic-assisted laparoscopic sacrocolpopexy with magnetic retraction: first experience using the SP da Vinci platform. J Robot Surg 2020;14:753-8.
30. Fulla J, Small A, Kaplan-Marans E, Palese M. Magnetic-assisted robotic and laparoscopic renal surgery: initial clinical experience with the Levita magnetic surgical system. J Endourol 2020;34:1242-6.
31. Chen W, Li Y, Qian R, et al. Application of a novel magnetic anchoring and traction technique in thoracoscopic esophagectomy: a swine experiment. Ann Transl Med 2021;9:1663.
32. Fu J, Li Y, Wang Z, et al. The role of magnetic anchoring and traction technique in thoracoscopic lymphadenectomy along the left recurrent laryngeal nerve. Surg Endosc 2022;36:3653-62.
33. Chen LH. 510(k) premarket notification. Available from: https://www.accessdata.fda.gov/cdrh_docs/pdf19/K191762.pdf [Last accessed on 17 Oct 2022].
34. Welsh LK, Davalos G, Diaz R, et al. Magnetic liver retraction decreases postoperative pain and length of stay in bariatric surgery compared to NATHANSON device. J Laparoendosc Adv Surg Tech A 2021;31:194-202.
Cite This Article
Export citation file: BibTeX | RIS
OAE Style
Romero-Velez G, Portenier D, Roberts J, Oviedo RJ, Rodriguez-Navarro A, Kroh MD. Magnetic-assisted surgery: the road from laparoscopy to robotics. Mini-invasive Surg 2022;6:56. http://dx.doi.org/10.20517/2574-1225.2022.51
AMA Style
Romero-Velez G, Portenier D, Roberts J, Oviedo RJ, Rodriguez-Navarro A, Kroh MD. Magnetic-assisted surgery: the road from laparoscopy to robotics. Mini-invasive Surgery. 2022; 6: 56. http://dx.doi.org/10.20517/2574-1225.2022.51
Chicago/Turabian Style
Romero-Velez, Gustavo, Dana Portenier, Jay Roberts, Rodolfo J. Oviedo, Alberto Rodriguez-Navarro, Matthew D. Kroh. 2022. "Magnetic-assisted surgery: the road from laparoscopy to robotics" Mini-invasive Surgery. 6: 56. http://dx.doi.org/10.20517/2574-1225.2022.51
ACS Style
Romero-Velez, G.; Portenier D.; Roberts J.; Oviedo RJ.; Rodriguez-Navarro A.; Kroh MD. Magnetic-assisted surgery: the road from laparoscopy to robotics. Mini-invasive. Surg. 2022, 6, 56. http://dx.doi.org/10.20517/2574-1225.2022.51
About This Article
Special Issue
Copyright

Data & Comments
Data
0

 Cite This Article 10 clicks
Cite This Article 10 clicks

 Like This Article 29
likes
Like This Article 29
likes






Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.